
Diastasis Rectus Abdominus (DRA): Mythbusting and Beyond

Diastasis Rectus Abdominus (DRA) AKA Diastasis Recti has been a hot topic in the fitness and wellness space. If you have heard about it, you are probably confused and perhaps even fearful of what you “should” or “shouldn’t” be doing. There is a lot of misinformation about what is “safe” or “unsafe” for exercise during pregnancy and postpartum and what might prevent abdominal separation, as well as myths about what can help resolve it. So here is some myth busting (based on the available evidence in 2023) to help you navigate what is often conflicting advice!
Take note → You can progressively train your core in all the ways! Consider adapting or modifying an exercise if you experience hard/firm doming. Keep reading for more on soft vs hard doming, myth busting, and progressive exercise!
Definition of DRA
Let’s get a bit nerdy!
Diastasis Rectus Abdominus is the formal name for abdominal muscle separation. DRA (“diastasis” for short) is a normal, physiological adaptation during pregnancy in nearly 100% of those in the 3rd trimester. This is your body making space for baby! Roughly 45% of those postpartum will still have some abdominal separation beyond what is considered “normal” at 6 months, and 33% at 12 months. Diastasis is not the same as a hernia, but they can co-occur.
“Diastasis recti abdominis is defined as an impairment with midline separation of the two rectus abdominis muscles along the linea alba.” (Bo et al 2017) Your “rectus” muscles are your “six-pack” muscles!
The linea alba is an incredibly strong 3-layered collagen structure along the midline abdomen to which other structures (such as the “sheath” around the rectus abdominus muscles) attach. While many think that diastasis is a disruption of the linea alba, it is a separation of the rectus muscles from each other, rather than an injury to the linea alba. (Axer et al 2001)
IRD (or inter-recti distance) is the distance between the two muscle bellies. This is frequently what practitioners measure when assessing DRA. There is no international agreement on what IRD is considered “normal” and what is considered “diastasis.” The German and European Hernia Societies suggest that Mild DRA is 2-3 cm, Moderate is 3-5 cm, and Severe is >5 cm.
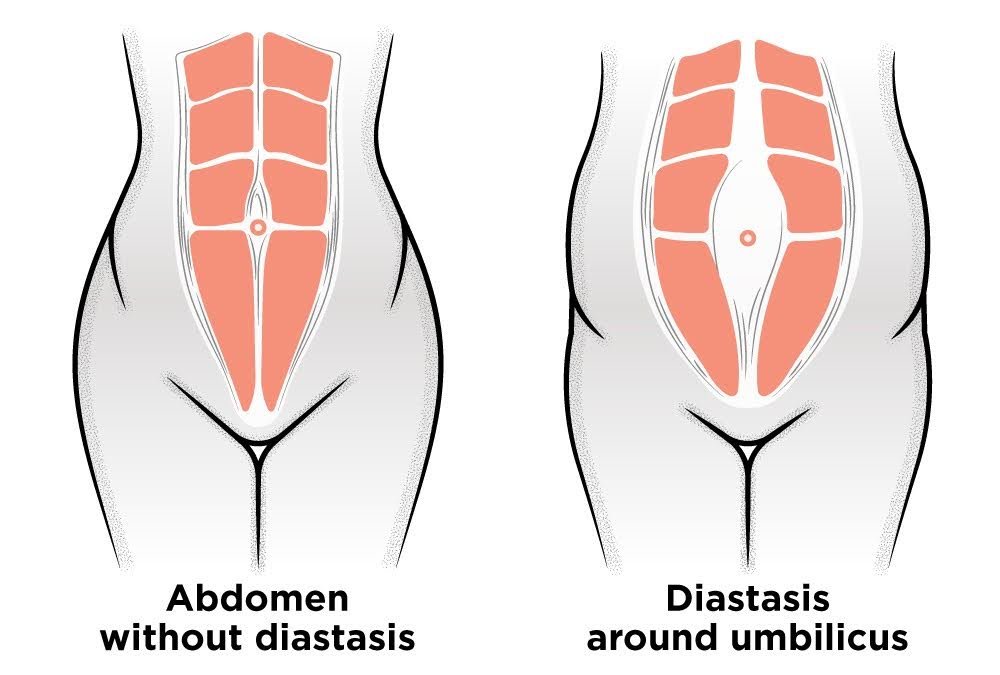
DRA can take place at different points along the midline. Some may have a separation above the umbilicus (navel, aka belly button), at the umbilicus, below the umbilicus, or even along the whole length of the midline. Some do not have what qualifies as a moderate or severe separation, and they still feel like they look pregnant. The shape of the abdomen can change for a lot of reasons, not just DRA. Genetics, GI dysfunction such as bloating, and previous or current weight gain can all affect the look and function of the abdominal wall.
About measuring DRA: The most accurate method of measuring DRA is via ultrasound imaging. Measuring with finger-widths or with calipers is not very reliable; however, this is frequently used in the clinic due to a lack of access to ultrasound. Know that it’s okay if you are measured this way, and it’s not essential to have imaging performed to achieve improvements to strength, function, and even aesthetics of the abdominal wall.
Mythbusting Diastasis
Myth: If you do enough (or the “right type”) of rehab/training, you can avoid or completely resolve diastasis.
Truth: We do NOT have evidence that shows that certain types of exercise or certain movements are harmful/will cause diastasis.
Truth: We do NOT have evidence that avoiding some types of exercise or avoiding doming/coning will prevent diastasis.
Truth: We do NOT have evidence that certain types of exercise are better for resolving diastasis. (But we have TONS of evidence of the general benefits of exercise!)
Myth: “Crunches” and rotation exercises should be avoided during pregnancy and postpartum if you have diastasis.
Truth: Refer to above! Also, studies are showing that abdominal curl-ups (aka crunches, sit ups, V-ups) do NOT make DRA better/worse, but do improve muscle strength and muscle bulk and improve the perception of DRA. (Gluppe, Engh, Bø 2023) What does “improves the perception of DRA” mean? This means that the individuals in the study who were doing curl-up exercises felt better about the look and function of their abdomen, even though the actual separation between the rectus muscles did not reduce.
Take Action: Performing exercises that “bulk up” the rectus muscles might actually help diastasis because it “fills out” the sheath (the tissue that surrounds the six-pack muscles, that the linea alba attaches to) of the muscle.
→ Have we been restricting the very exercises that might be the most helpful?? 🤔
Myth: Diastasis is associated with pelvic floor dysfunction.
Truth: Evidence does not appear to show any association (meaning one comes along with the other) for diastasis and pelvic floor dysfunction. In fact, those with diastasis actually show lower rates of pelvic organ prolapse (POP) than those without diastasis. (Bø et al., 2017) In that study, rates of POP were 4x higher for those without diastasis. (DRA is a natural adaptation during pregnancy and early postpartum that might be protective?!)
Myth: You should wear an abdominal binder or support to help diastasis resolve.
Truth: A large systematic review (high level of evidence!) from Benjamin et al., 2023 found NO BENEFIT from using abdominal binders, kinesiotape, or manual therapies for decreasing inter-recti distance (IRD: the amount of distance between your two rectus abdominal muscles).
→ Now for a bit of nuance: While this means binders are not likely to help reduce an abdominal separation, there may be other reasons you use these treatments such as they reduce pain or discomfort (especially for cesarean or abdominal surgeries) or they help you feel more comfortable in your current body, and that’s ok!
Take Action
So if we don’t know what type of exercise causes diastasis, and we don’t know exactly what makes it better, what can we do about it?
Well, for one, we can stop restricting our exercise for fear of “making things worse” or causing diastasis. We have the highest levels of evidence supporting the safety and benefit of exercise, including cardiovascular and strength training, even during pregnancy for those not high-risk. Reducing or limiting exercise may have negative unintended consequences. Also, we can be mindful of how we exercise, meet ourselves at our current levels of fitness, and make adjustments along our pregnancies and postpartum journeys.
Some of the many benefits of exercise for DRA:
Improves strength
Improves function (ability to perform everyday tasks with greater ease- like lifting heavy car seats, wiggly children, etc!)
Improves body image and perception of DRA
Many also see aesthetic benefits, take note that these often take the longest to notice
>> You need to LOAD tissues appropriately to cause change (“LOST” principle: Load Over Specific Time) and you need to do it CONSISTENTLY! That’s the hard part. Many don’t see/feel change as quickly as they’d like and they give up or move to the next thing.
What is an “appropriate load”? Find a load that meets you where you are, but is challenging, and train consistently, 3-5 days a week. If you don’t feel challenged, you likely aren’t driving adaptive change. Laying on your back doing “deep core activation” may have a place right after birth or surgery, but this likely will not be enough to improve DRA.
Consider using “Reps in Reserve” to find an appropriate level of challenge. If you do a round of movements and could easily keep going (say 10 more reps), chances are you need to increase the challenge in some way (by adding load or reps, or a more challenging position). Conversely, if you are barely able to eek out the last rep or you are experiencing unwanted pain or pelvic discomfort, you might dial the challenge back. See the doming/coning section below for more on this!
🔑How many reps, sets, etc!? There are many different types of programming options, the best one is the one that you will do! Remember: There are no evidence-based preferred (no “RIGHT/WRONG”) exercise progressions/movements. Seriously.
TRAIN “ALL THE WAYS”: Exercise should be progressive (increasing challenge & volume over time) and also address the main ways we use our abdominal muscles to move and carry loads. Here is your friendly reminder that SP programming has “core exercise” built into it! Some examples of commonly programmed movements from our Daily Workouts:
Trunk Flexion/Extension: V-ups, Kipping Pull Ups, Toes to Bar, Sit Ups, Plank/Push Ups
Trunk Rotation and Anti-Rotation: Turkish Get Ups, Renegade Rows, single-arm movements like Single Arm KB/DB Shoulder Rack Step Ups, Push Up Pull Across
If you want even more core, check out the Butts & Guts Extra Programs on the app or my.streetparking.com website under Train > Extra Programs > Strength.
While we don’t have a “diastasis-specific” program, we have programs that can provide you with a progressive structure. Check out our Rehab and Rebuild programs, which were created as a postpartum program to bridge our Recovery program with SP SHIFT or Programs A, B, and C. Even though they were made as postpartum programs, they are progressive core function programs that can be used for DRA and/or abdominal surgery rehab. If you have any questions on which program would be best for you to start, feel free to email mamas@streetparking.com.

What About Doming/Coning?
Doming, coning, and bread loafing (among others) are names for the abdominal wall protruding at the midline, typically during movement and exercise. As early as five years ago (and these messages persist today), it was incredibly common to hear that ANY movement that caused doming was an indicator that a movement was “too much” challenge for the abdominal wall and that doming would cause diastasis. Much of this was based on theory and hypothetical risk. While the evidence on the effect of coning is still pretty limited, the theories about doming/coning have become a more nuanced conversation.
The current thinking from many of the world’s leaders in diastasis rehab suggests that doming/coning is more of a spectrum. Consider the spectrum of doming/coning along the lines of softer ↔ harder/more firm (acknowledgment to Antony Lo for this concept).
Soft doming that can easily be pressed into is thought to be unlikely to cause permanent stretch or “damage” to the tissues. To “overstretch” something, you must take it to its end range and sustain that over time.
To illustrate that concept, imagine a rubber band that is being held by your hands with some slack in it. If you were to move your hands apart so that the slack is taken out of the rubber band but there is no stretch or even a minimal amount of stretch, do you think that amount of resistance on the rubber band would cause it to become stretched out? Probably not. You might consider soft doming to be like taking the slack out of the tissue that separates the rectus abdominus, or “six-pack” muscles. Keep in mind, this is not a perfect analogy. Our bodies are not purely mechanical like a rubber band, but rather living tissues capable of adaptation, and our tissues can react positively to loads and stretch. This analogy is simply to demonstrate the concept.
What does soft or hard doming feel like? Press into your cheek — this is soft. Firm doming feels more like pressing into the tip of your nose.
If after reading this you decide you just don’t like how doming looks, don’t want people commenting, or do not feel comfortable allowing soft doming to be present in your abdomen during exercise, that’s ok! There are plenty of ways to adjust and adapt your exercise within your level of comfort. Remember to refer to the “Strategies Videos” in the Mamas’ Movement Library for ideas on how to adjust breath, position, posture, impact during exercise. Try different things, and see what feels better or softens/reduces your doming. You might not need to make a movement or exercise “easier” to soften or reduce doming/coning, you may be able to modulate or change the doming with a breathing or position strategy. Some examples: You might try an exhale or a “ribs wide” cue during a movement such as a hollow hold or pull up. Some may find they can control their abdominal wall better using a breath hold. An example of a positional strategy is not leaning as far during the pull when on the rower. Again, there is no perfect way to perform these movements — explore and see what works for you.
A note on aesthetics…
There are other reasons you might notice changes to the look and function of your abdomen after pregnancy, with or without DRA. Everyone is different with regards to how much they will experience stretch marks, loose skin, or even a general widening of the abdomen. Most of this is due to genetic factors beyond our control. There are those who can do every rehab program and be the same body composition as they were pre-pregnancy, and they might still desire aesthetic changes, and that’s okay.
Keep in mind as you progress through the Fourth Trimester bundle (or whatever exercise plan you follow) that aesthetics are typically the slowest to change. There is SO MUCH you can do to continue to get strong and to be able to do the movement and exercise that you want to do!
What About Surgical DRA Repair?
Surgery for DRA does not have to be a “last resort,” something you need to “earn” or receive permission to consider. Here are a few more myths that need busting!
Myth: If you decide to have surgery you are “taking the easy way out.”
Truth: Diastasis repair surgery/tummy tuck recovery is NOT easy. Also, there are benefits from getting as strong as possible both before and after surgery, so rehab efforts are never “wasted.”
Myth: If you do enough (or the “right type”) of rehab/training, you can avoid surgery (therefore, if you have surgery you “failed” rehab).
Truth: Some people will not achieve the aesthetic changes they desire no matter how much they exercise. Much of this is largely the genetic luck of the draw. That does not mean we have no control over the outcome.
Truth: We’ve said it before and we’ll say it again: we do not have evidence showing us that specific types of training will yield certain aesthetic results.
Myth: DRA repair/abdominoplasty will always yield a perfectly flat and aesthetically pleasing abdomen, will resolve all psychosocial aspects of DRA.
Truth: There are often “ups and downs” following surgery with regards to bloating, aesthetic changes over time, as well as certain aspects of surgery that individuals may not be pleased with (such as scarring).
Truth: People often report finding they still have some emotional and mental things to work through following surgery. Seek counseling or emotional support as needed!
Some things to think about if you are considering surgery:
Can you/your family shoulder the financial burden?
How will you manage (your work, household, children, etc.) in the postoperative period?
What are your expectations of surgery?
What are your goals?
How can you bolster your mental health during and after surgery?
You can expect very low function in the initial post-op period. The first few weeks after a DRA repair surgery are typically focused on pain control and sitting/laying/standing gradually in a more upright position. You will likely be unable to care for young kids, do housework, or perform job duties (of course this depends on what they are and those with less physical jobs are often able to return to work earlier than those with heavier physical demands).
You will also be unable to exercise as usual, initially. This might lead to challenges with mental health, especially if you use exercise as a way to manage stress and anxiety. In 2017, Weinstein et al published a systematic review (very high level of evidence!) which concluded that in healthy adults, “experimentally controlled exercise withdrawal consistently resulted in increases in depressive symptoms and anxiety…with stronger effects if exercise withdrawal exceeded two weeks.”
Street Parking’s Fourth Trimester Bundle is a fantastic program to follow after Diastasis Repair surgery. Consider waiting 2-3 weeks to begin the very gentle yet progressive “Recovery” program, available to all Street Parking members with an active membership. Then you can start the “Rehab” program once your surgeon clears you to begin exercise. Then comes “Rebuild,” which will help to bridge you back to Street Parking SHIFT or Programs A, B, and C! Both Rehab and Rebuild are available as a “bundle,” which is an additional purchase to the regular SP membership. There is lifetime access so long as there is an active membership.
The exact timelines for recovery following DRA repair will vary greatly. Be sure to follow your surgeon’s guidance following surgery!
This is not necessarily an exhaustive list of things to consider before deciding on surgery or a surgeon. If you would like more information and support as well as a program specific to DRA repair, our colleagues Lisa Marie Ryan and Munira Hudani over at Tummy Tuck Rehab have some great resources. Check them out over at www.tummytuckrehab.com.
A note on fatigue and rest…
Do not underestimate the impact of fatigue on your recovery! You may need to dial things back (with regards to load, intensity, challenge, etc) if you are not recovering well or experience excessive fatigue, pain, swelling, or other unwanted symptoms in the day or two following a movement session. Observe the body’s response to new training stimuli, movements, or demands and make adjustments as needed. You may experience symptoms as you introduce new movements, loads, volume, intensity, etc. Note in your Logbook and remember to keep using your strategies to help you assess and adjust.
In Summary
While ‘do this/ don’t do that’ advice regarding exercise may be well-intended, research does not support limiting certain activities or movements in the prenatal or postpartum time frame. There are no research-supported best exercises for DRA rehab. We suggest a well-rounded, progressive strengthening program that is SIMPLE enough to get done but NOT EASY — you need to be challenged to drive adaptive change! Consider customizing or modifying an exercise if you experience hard/firm doming. If you still have questions and concerns, consider seeking support from a trusted rehab or fitness provider for individualized advice, and reach out to us as needed at mamas@streetparking.com.
Even incredibly strong people can have abdominal separation!

Ronnie Coleman 8x Mr Olympia
Photo by: www.localfitness.com.au
License: CC BY-SA 3.0 DEED